Author: Eshwar Cherkuri
📍Las Positas College
Introduction
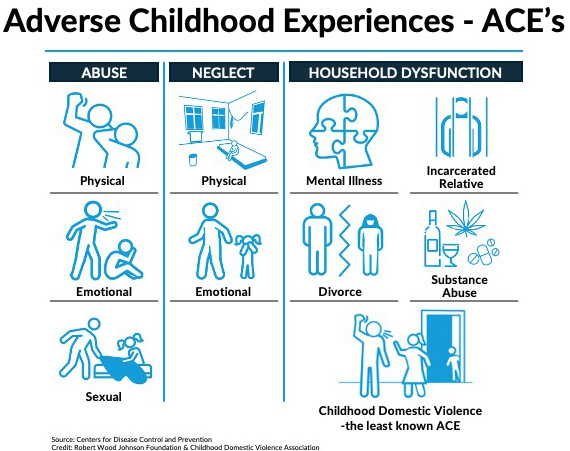
Adverse Childhood Experiences (ACEs), which include physical and emotional abuse, neglect, or witnessing violence during early childhood, have profound psychological impacts lasting into adulthood, such as preventing people from attaining long-term financial stability. These early forms of trauma greatly increase the likelihood of the children developing chronic illness, substance use, and emotional disorders, which also further systemic barriers these children face for social mobility and financial stability (CDC-Kaiser Permanente ACE Study). Victims of nonfatal child maltreatment are estimated to face a lifetime cost of $831,000 per victim, while those resulting in death cost $16.6 million per victim (Fang et al., 2012). These costs include estimates of health care costs, child welfare costs, criminal justice costs, and special education costs; each is considered but may have limitations due to the insufficient sample of children studied and changing economic factors like inflation (Fang et al., 2012). Apart from the direct health cost, ACEs are leading causes of chronic conditions like heart disease, diabetes, and mental illness. From a study undertaken by the JAMA Network (2023), it was estimated that ACEs were responsible for causing 55% of smoking cases, which amounts to an annual financial burden of $4.1 trillion for smoking-related illness alone.
Furthermore, mental illnesses like depression are very prevalent results of childhood trauma that cost approximately $50 billion a year in medical costs (Merrick et al., 2015-2017). Despite the supposed availability of mental healthcare, bureaucratic regulations and stigmatism prevent effective treatment for trauma victims of ACEs because those services are not readily advertised or accessible to the victims. For example, in 2015, there were 1.6 million children in California who were witnesses or victims of community violence, and only 35 compensation claims were filed for trauma-related mental health treatment (Gilad, 2015). This discrepancy shows how bureaucratic systems fail to provide adequate support and care for those who struggle with years of childhood trauma, especially the low-income families who struggle most with the issue and have the most trouble seeking support to fix it. The lack of intervention has repercussions that put victims in greater danger of committing crime, homelessness, and the continuation of cycles of poverty.
A. School Dropout Rates and Obstacles to Education
ACES impacts academic performance and school retention by increasing absenteeism, behavioral problems, and educational underachievement (Dyregrov, 2004). Recurring exposure to excessive stress usually leads to psychiatric issues such as anxiety, depression, or PTSD, resulting in greater school disengagement (Shnurr, Friedman, & Bernardy, 2002). Furthermore, Psychiatric disorders often result from prolonged exposure to high levels of stress, whether from domestic abuse, neglect, or instability at home, causing students impacted to become disengaged from school and feel alienated from learning environments (Shnurr, Friedman, & Bernardy, 2002). In this vulnerable state, students often display “disorganized” or “agitated” behavior, which educators frequently interpret as deliberate misconduct that can be solved through school punishments. Instead of seeing these actions as indicators of emotional distress, schools tend to use harsh discipline methods in response. Students who have experienced trauma are disproportionately impacted by the strict implementation of zero-tolerance policies, which impose severe penalties for defiance or drug use. In addition to further isolating vulnerable adolescents from education and intensifying their emotional and developmental difficulties, these practices frequently lead to suspensions, expulsions, or even school-based arrests (American Psychological Association Zero Tolerance Task Force, 2008).
B. Long-term workforce and economic effects
Child trauma has a long-term impact that carries through to adulthood and affects work and financial standing. “It disrupts brain architecture, affects other organ systems, and leads to stress-management systems that establish relatively lower thresholds for responsiveness that persist throughout life, thereby increasing the risk of stress-related disease and cognitive impairment all into the adult years” (Shonkoff et al., 2009). This has a cascading effect and leads to victims of child maltreatment having lower wages and schooling by considerable margins (Metzler et al., 2020). School dropouts, a common outcome for trauma-exposed students, are paid thirty-five percent less and are twice as likely to remain unemployed. Additionally, ACE victims experience higher rates of substance abuse, mental illness, and crime, and are also restricted in many socio-economic avenues. Early trauma is highly correlated with diminished educational attainment, and this leads to restricted access to steady income and financial autonomy (Gilbert, 2020). If left without focused intervention, this forms intergenerational cycles of poverty that serve to keep them stuck at a socio-economic disadvantage.
C. Socioeconomic Determinants Contribution to Trauma Prevalence and Recovery
ACEs affect children with low-income backgrounds disproportionately, and these children have greater poverty and housing instability, which further intensifies chronic stress and emotional instability. Poor children receive less medical treatment, and due to disadvantages such as higher poverty and housing instability, they are more prone to maltreatment and abuse (Berger, 2004; Putnam-Hornstein & Needell, 2011). While adversity in early childhood may create resilience and learning to grow into adulthood, this can be achieved by making mistakes and learning from them with guidance from parents or adults who have not experienced traumatic events that have long-lasting effects. In children with ACEs, however, resilience was more likely to be consciously built through support mechanisms rather than through a parent or guardian (Greenberg, 2006).
Race and socioeconomic status apply to long-term trauma impact based on difficulty with fitting into colleges and universities, and with the community, with individuals, and being discriminated against by younger children who do not know how to be respectful. One study of 1,000 children in high-risk communities found that Black children with families that are still quite affluent were still more subject to trauma by systemic discrimination and violence in communities (Gilbert, 2020). In contrast to white children with higher incomes, Black children with higher incomes are more susceptible to peer violence in segregated school communities and to drugs and bad schooling. These disparities are a sign of decreased protection effects of socioeconomic mobility for minority groups and show that culturally competent trauma services are necessary. Unless these disparities are addressed, there will still be racial disparities affecting minorities in recovery from trauma and financial achievement.
D. Solutions
Although some state policies have increased awareness of ACEs, many do not address structural causes such as poverty, discrimination, and inadequate access to healthcare (ScienceDirect, 2021; Prewitt, 2014). Government interventions like Medicaid expansion have improved parental access to substance abuse and mental health treatment, reducing child maltreatment risks (Alderson & Morrow, et al.). Similarly, the Family First Prevention Services Act of 2018 allocates federal funding to keep families with children together to reduce unnecessary foster care placement (Garcia Caitlyn, 2021). The strategy uses public-private partnerships that utilize neuroscience and research through training school teachers, working with community centers, and utilizing health institutions to increase awareness about ACEs and train crucial workers to minimize the effects on children. California’s trauma-informed schools plan, which incorporates mental health services into public education, is another encouraging policy model. According to the California Department of Education, schools that provided staff with trauma-sensitive training reported higher attendance and fewer suspensions. Furthermore, public-private partnerships, like Tennessee’s Building Strong Brains program, which trained over 80,000 healthcare professionals and 7,000 educators, integrate neuroscience research into public service training. This shows how programs can prepare schools, hospitals, and community organizations to respond to childhood trauma effectively. A national expansion of such models, particularly in high-poverty districts and juvenile justice programs, could reduce suspensions, improve mental health outcomes, and improve the financial standings of impacted children significantly.
References
Alderson, P., & Morrow, V. (2011). The ethics of research with children and young people: A practical handbook.
Berger, L. M., & Putnam-Hornstein, E. (2020). Family structure, socioeconomic status, and child abuse risk. Child Abuse &
Neglect, 106, 104512. https://doi.org/10.1016/j.chiabu.2020.104512
Dyregrov, A. (2004). School dropout and trauma. Journal of Loss and Trauma, 9(1), 63–69.
Fang, X., Brown, D. S., Florence, C. S., & Mercy, J. A. (2012). The economic burden of child maltreatment in the United States
And implications for prevention. Child Abuse & Neglect, 36(2), 156–165.
Fratto, C. M. (2018). The Family First Prevention Services Act: Historic reforms to the child welfare system.
Garcia, C. (2019). Replacing foster care with family care: The Family First Prevention Services Act of 2018. Family Law
Quarterly, 53(1/2), 27–49.
Gilad, M. (n.d.). Childhood exposure to trauma costs society $458 billion annually. Penn Today.
Gilbert, R., Widom, C. S., Browne, K., Fergusson, D., Webb, E., & Janson, S. (2020). Burden and consequences of child
Maltreatment in high-income countries. European Child & Adolescent Psychiatry, 29(9), 1123–1134.
Metzler, M., Merrick, M. T., Klevens, J., Ports, K. A., & Ford, D. C. (2016). Adverse childhood experiences and life
Opportunities: Shifting the narrative. Children and Youth Services Review, 72, 141–149.
National Governors Association. (n.d.). State actions to prevent and mitigate adverse childhood experiences.
